
Krieger N, Kiang M, Chen J, Waterman P. Trends in U.S. deaths due to legal intervention among black and white men. Harvard Public Health Review. Winter 2015;3. 10.54111/0001/C4
To inform current national discussions about the deaths of black men due to the police, we present novel data on long-term trends (1960-2010) in deaths due to legal intervention (i.e., deaths due to law enforcement actions) among US black and white men, by county income level. Among the three health studies investigating trends in this outcome, one focused on the total US population for 1962-1993, one documented a marked excess for young adult black as compared to white men for 1979-1997, and the third reported on systematic underreporting of such deaths, overall and by race/ethnicity and age, for 1976-1998; none included socioeconomic data.
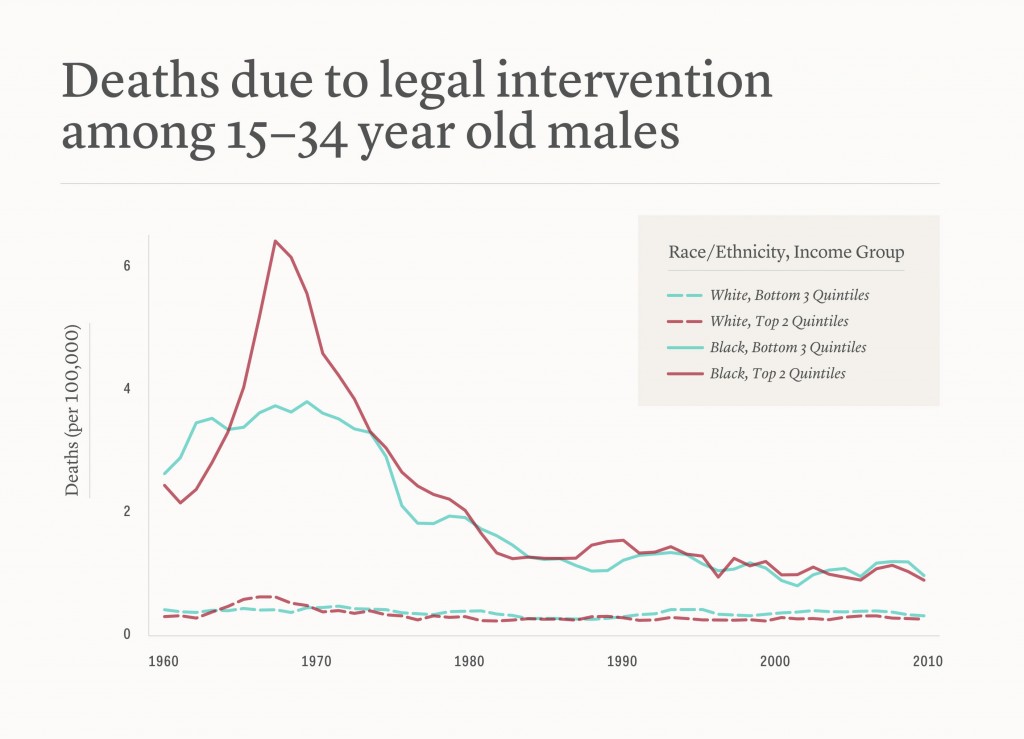
We analyzed US national mortality data for 1960-2010, using individual-level mortality records and census denominator data stratified by age, gender, and race/ethnicity, aggregated to the county level, and to which we have appended the corresponding year-specific US county median family income data, categorized into quintiles. We report trends (3-year moving average mortality rates) for the two main groups at risk: US black and white men, age 15-34.
Between 1960 and 2010, 15699 US deaths were classified as due to legal intervention, of which 63.3% (n=9934) occurred among men age 15-34. Among these men, 5489 were classified as white (55.3%) and 4204 as black (42.3%), a percentage 3 to 4 times that for the US black population (e.g., 1960: 10.5% black, 88.6% white; 2010: 12.6% black, 72.4% white). Only rates for the black men exhibited a sharp rise and fall (1960s-1970s) followed by a post 1980-plateau; rates for the white men exhibited far less variation (Figure 1, Table 1). The rate ratio for black vs. white men for death due to legal intervention always exceeded 2.5 (median: 4.5) and ranged from 2.6 (95% confidence interval [CI] 2.1, 3.1) in 2001 to 10.1 (95% CI 8.7, 11.7) in 1969, with the relative and absolute excess evident in all county income quintiles (Table 1).
Our results indicate that the excess black vs. white mortality rate among men age 15-34 due to legal intervention is both longstanding – and modifiable. Given documented greater underreporting of black vs. white homicides by police officers, the results also likely underestimate the black vs. white excess. Moreover, the lack of sharp difference by county income quintile, post-1980, stands in contrast to well-documented inequities by county income level for both infant mortality and premature mortality (death before age 65), suggesting that societal determinants of deaths due to legal intervention are driven by additional or different aspects of societal inequality. We cannot, based on the limited data available, address debates over whether our findings reflect racially biased use of excessive force. Nevertheless, the data presented provide context for the 2014 emergence of police killings as a highly visible topic. Repeated protests have taken place in most major US cities, about both the deaths themselves and also – in the two very high profile cases involving Michael Brown (Ferguson, Missouri) and Eric Garner (Staten Island, New York) – the decision of grand juries to decline recommending that criminal charges be filed for these deaths. Journalists report that these latest deaths and the responses of the criminal justice system have reignited the concerns and distress triggered by the 2012 acquittal of George Zimmerman, a volunteer neighborhood watchman who killed the teenager Trayvon Martin. In all three of these cases, the victims were unarmed Black American teenage boys or men. The dearth of health research on police killings and their impact on the families, neighborhoods, and communities affected is stark. When it comes to reckoning the toll of racial inequality, accountability requires counting. We offer these descriptive analyses to stimulate further investigation into the patterns, causes, and consequences of social inequalities in deaths due to legal intervention.
US mortality rates (3-year moving average, per 100,000), and rate ratio and rate difference (and 95% confidence interval (CI)), for black and white men, ages 15-34, for deaths due to legal intervention, overall and by county income quintile: 1965, 1975, 1985, 1995, and 2005
| Year | Group | Death due to legal intervention | |||
|---|---|---|---|---|---|
| Rate | Rate ratio | Rate difference | |||
| Black | White | RR (95% CI) | RD (95% CI) | ||
| 1965 | Total | 3.33 | 0.44 | 7.65 (6.48, 9.02) | 2.90 (2.51, 3.28) |
| Income quintile: | |||||
| Q1 (low) | 2.33 | 0.36 | 6.45 (4.30, 9.72) | 1.97 (1.35, 2.59) | |
| Q2 | 4.78 | 0.35 | 13.60 (9.44, 19.76) | 4.43 (3.38, 5.48) | |
| Q3 | 3.36 | 0.51 | 6.57 (4.59, 9.38) | 2.85 (2.00, 3.69) | |
| Q4 | 3.21 | 0.59 | 5.47 (3.78, 7.84) | 2.62 (1.72, 3.52) | |
| Q5 (high) | 3.43 | 0.36 | 9.61 (6.15, 14.93) | 3.07 (2.01, 4.14) | |
| 1975 | Total | 2.96 | 0.39 | 7.56 (6.52, 8.77) | 2.57 (2.26, 2.87) |
| Income quintile: | |||||
| Q1 (low) | 2.27 | 0.45 | 5.03 (3.63, 6.98) | 1.82 (1.31, 2.33) | |
| Q2 | 3.33 | 0.38 | 8.67 (6.29, 11.99) | 2.94 (2.26, 3.62) | |
| Q3 | 3.53 | 0.44 | 8.02 (5.68, 11.25) | 3.09 (2.19, 3.99) | |
| Q4 | 3.37 | 0.38 | 8.93 (6.50, 12.31) | 3.00 (2.30, 3.69) | |
| Q5 (high) | 2.46 | 0.30 | 8.13 (5.21, 12.53) | 2.16 (1.36, 2.95) | |
| 1985 | Total | 1.25 | 0.28 | 4.48 (3.71, 5.39) | 0.97 (0.79, 1.15) |
| Income quintile: | |||||
| Q1 (low) | 0.91 | 0.29 | 3.08 (1.98, 4.75) | 0.61 (0.31, 0.91) | |
| Q2 | 0.86 | 0.22 | 3.87 (2.28, 6.43) | 0.64 (0.30, 0.98) | |
| Q3 | 2.03 | 0.34 | 6.03 (4.24, 8.58) | 1.69 (1.19, 2.19) | |
| Q4 | 1.37 | 0.31 | 4.46 (2.98, 6.62) | 1.06 (0.65, 1.47) | |
| Q5 (high) | 1.08 | 0.23 | 4.61 (2.63, 7.80) | 0.84 (0.38, 1.31) | |
| 1995 | Total | 1.21 | 0.36 | 3.37 (2.81, 4.02) | 0.85 (0.68, 1.02) |
| Income quintile: | |||||
| Q1 (low) | 1.10 | 0.57 | 1.94 (1.35, 2.77) | 0.53 (0.20, 0.87) | |
| Q2 | 0.96 | 0.26 | 3.73 (2.30, 5.98) | 0.71 (0.35, 1.06) | |
| Q3 | 1.43 | 0.47 | 3.04 (2.11, 4.33) | 0.96 (0.55, 1.36) | |
| Q4 | 1.41 | 0.31 | 4.56 (3.02, 6.83) | 1.10 (0.67, 1.53) | |
| Q5 (high) | 1.13 | 0.21 | 5.49 (3.19, 9.27) | 0.92 (0.48, 1.37) | |
| 2005 | Total | 0.94 | 0.37 | 2.57 (2.12, 3.09) | 0.58 (0.43, 0.72) |
| Income quintile: | |||||
| Q1 (low) | 0.87 | 0.37 | 2.33 (1.54, 3.48) | 0.49 (0.21, 0.77) | |
| Q2 | 0.89 | 0.41 | 2.16 (1.42, 3.24) | 0.48 (0.17, 0.79) | |
| Q3 | 1.19 | 0.41 | 2.89 (1.93, 4.28) | 0.78 (0.40, 1.16) | |
| Q4 | 0.76 | 0.34 | 2.22 (1.35, 3.55) | 0.42 (0.11, 0.73) | |
| Q5 (high) | 1.09 | 0.30 | 3.65 (2.21, 5.89) | 0.79 (0.37, 1.21) | |
Nancy Krieger is Professor of Social Epidemiology, Department of Social and Behavioral Sciences, at the Harvard T.H. Chan School of Public Health and Director of the HSPH Interdisciplinary Concentration on Women, Gender, and Health. She has been a member of the School’s faculty since 1995. Dr. Krieger is an internationally recognized social epidemiologist (PhD, Epidemiology, UC Berkeley, 1989), with a background in biochemistry, philosophy of science, and history of public health, plus 30+ years of activism involving social justice, science, and health. In 2004, she became an ISI highly cited scientist, a group comprising “less than one-half of one percent of all publishing researchers, with her ranking reaffirmed in the 2015 update.” In 2013, she received the Wade Hampton Frost Award from the Epidemiology Section of the American Public Health Association, and in 2015, she was awarded the American Cancer Society Clinical Research Professorship, and re-awarded its renewal in 2020. In 2019, Dr. Krieger was ranked as being “in the top 0.01% of scientists based on your impact” for both total career and in 2017 by a new international standardized citations metrics author database, including as #1 among the 90 top scientists listed for 2017 with a primary field of public health and secondary field of epidemiology (https://doi.org/10.1371/journal.pbio.3000384). In 2020, she was awarded the American College of Epidemiology’s “Outstanding Contributions to Epidemiology” award, and she and her team received the 2020 American Journal of Epidemiology “Paper of the Year” award for their study on historical redlining and cancer stage at diagnosis (the first ever study on this issue). In 2021, she was appointed as member of the UNESCO International Scientific Committee for the Slave Route Project: Resistance, Liberty, Heritage.
Dr. Krieger’s work addresses three topics: (1) conceptual frameworks to understand, analyze, and improve the people’s health, including the ecosocial theory of disease distribution she first proposed in 1994 and its focus on embodiment and equity; (2) etiologic research on societal determinants of population health and health inequities; and (3) methodologic research on improving monitoring of health inequities. In April 2011, Dr. Krieger’s book, Epidemiology and the People’s Health: Theory and Context, was published by Oxford University Press. This book presents the argument for why epidemiologic theory matters. Tracing the history and contours of diverse epidemiologic theories of disease distribution from ancient societies on through the development of — and debates within — contemporary epidemiology worldwide, it considers their implications for improving population health and promoting health equity. She is also editor of Embodying Inequality: Epidemiologic Perspectives (Baywood Press, 2004) and co-editor, with Glen Margo, of AIDS: The Politics of Survival (Baywood Publishers, 1994), and, with Elizabeth Fee, of Women’s Health, Politics, and Power: Essays on Sex/Gender, Medicine, and Public Health (Baywood Publishers, 1994). In 1994 she co-founded, and still chairs, the Spirit of 1848 Caucus of the American Public Health Association, which is concerned with the links between social justice and public health.
Dr. Mathew V. Kiang, MPH, SD, is an Instructor in the Department of Epidemiology and Population Health at Stanford University School of Medicine and a Fellow at the Harvard FXB Center for Health and Human Rights. He received his doctorate in Quantitative Methods from the Department of Social and Behavioral Sciences at Harvard TH Chan School of Public Health. Before that, he received an MPH at New York University, my BA in Sociology from San Diego State University, and was a 2016 fellow at University of Chicago’s Data Science for Social Good summer fellowship. His research lies at the intersection of computational social science and social epidemiology. Methodologically, his work revolves around combining disparate data sources in epidemiologically meaningful ways.
Dr. Jarvis Chen is a social epidemiologist whose research focuses on social inequalities in health, and especially racial/ethnic and socioeconomic disparities in cancer outcomes. As a methodologist, Dr. Chen’s interests include the development of methods for geospatial and spatiotemporal analysis, disease mapping, handling missing data, and latent variable analysis.
Pamela D. Waterman, MPH, is a Project Director, at the Harvard T.H. Chan School of Public Health, in the Social and Behavioral Sciences.
HPHR.org was designed by ComputerAlly.com.
Visit HPHR’s publisher, the Boston Congress of Public Health (BCPH).
Email communications@bcph.org for more information.
Click below to make a tax-deductible donation supporting the educational initiatives of the Boston Congress of Public Health, publisher of HPHR Journal.![]()