Community Health Centers (CHC) began in Massachusetts. The first CHC was founded in Dorchester in 1965, to provide primary and preventative care to individuals without health insurance (MLCHC, 2019). Massachusetts now has 285 CHCs providing care to more than 950,000 individuals (MLCHC, 2019). CHCs were created with the goal of providing all levels of care including preventative, primary, and chronic, that is accessible to those who are Medicaid insured or uninsured. When the Affordable Care Act (ACA) was enacted in 2010, it helped expand the number, and services, of CHCs by increasing funds for federally qualified community health centers (FQCHC). Through increasing access to preventative care, another beneficial effect of increasing CHCs may be a decrease in unnecessary or preventable emergency department (ED) usage. Decreased ED usage results in large financial savings from things such as effective management and prevention of chronic conditions. There is a lack of research concerning ED and CHC usage in Massachusetts since the ACA increased funding for FQCHC, and services provided. This literature review will examine FQCHCs, CHCs, and ED’s throughout the United States during the time of the ACA to compare Massachusetts FQCHCs, CHCs, and ED usage.
The price of healthcare has increased dramatically in recent years, totaling 17% of the US gross domestic product in 2017, and is expected to continue rising (Du, 2018). Approximately $8.3 billion of healthcare expenditure is spent on unnecessary ED visits (Premier, 2019), a cost that has more than doubled since the estimated $4.4 billion in 2010 (Weinick, 2010). This is largely due to usage from individuals who do not qualify for Medicaid, but cannot afford to purchase private insurance. The ACA expanded Medicaid eligibility in 2010 by allowing states to determine if individuals living above the federal poverty line could enroll. Though the expansion helped, there were still 500,000+ individuals left without health insurance in 2018 (Tolbert, 2019). Without access to preventative and primary care, along with the lack of urgent care clinics available, individuals are more likely to use the ED as a “safety net” clinic (Nath, 2019).
Medicaid insured individuals without access to a primary care provider taking Medicaid patients have little to no options besides the ED as well. Even though these individuals are insured, the unnecessary usage increases debt. For example, an individual who is Medicaid insured and goes to the ED for any non-emergent cause would only be charged $8 (CMS, 2013). The American College of Emergency Physicians found that approximately 50% of ED admissions go uncompensated, and one in five patients treated in the ED has no form of health insurance (American College of Emergency Physicians, 2013). With the average price of an ED visit in 2014 being $1,533, it is clear why healthcare is accruing so much ED related debt, especially when the primary users are uninsured, and Medicaid insured persons. CHCs and FQCHCs can help reduce the high costs stemming from unnecessary and preventable ED usage, when utilized by the correct populations. Dr. Basu found that only 4-5 less ED visits per provider per year would make CHCs financially neutral, or even beneficial (Basu, 2017). This is a very attainable goal when individuals are given access to primary care providers and able to treat their chronic conditions.
CHCs and FQCHs offer both primary and specialty services including dermatology, maternal and child health services, smoking cessation programs, family medicine, among others to provide effective primary, secondary, and tertiary prevention and decrease preventable ED usage (MLCHC, 2019). The services offered at a CHC vary depending on a populations’ needs in a given area, though most clinics provide similar preventative programs such as HIV screening and counseling, along with nutrition counseling. These programs are consistent among CHCs due to the common health problems associated with populations experiencing more social determinants of health. The ACA increased funding for these types of prevention programs, and recent studies have found that these community and case-management focused interventions help lower hospital admissions, readmissions, and ED usage (Berkowitz, 2018; Raven, 2016; Grazioli, 2019). One study found that within 3 years of states increasing funding to CHCs, uninsured ED visits decreased by 40%, saving hospitals an estimated $14 million (Smith-Campbell, 2019). Proper management of chronic conditions through CHCs can significantly reduce preventable ED usage and accrue large cost savings. Another study focusing on end stage kidney disease discovered when patients receive dialysis on a routine basis it costs $207,759 less per person than an individual using the ED for emergency only dialysis (Sheikh-Hamad, 2007).
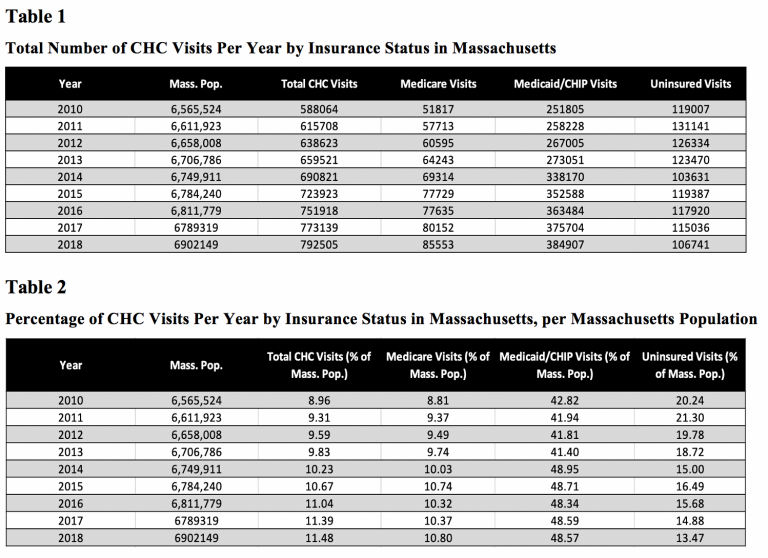
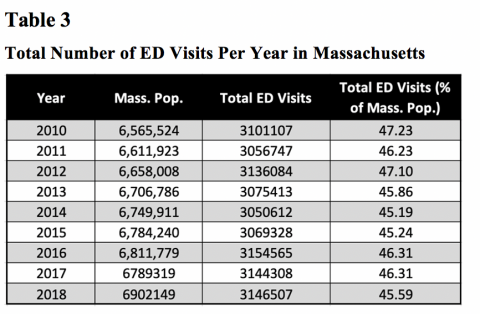
It is important to have a large network of CHCs providing a range of services as well. The individuals utilizing these clinics are primarily of low socioeconomic status, so barriers such as access to transportation must be considered. Massachusetts’s 285 CHCs are spread across the state consistently, with the number of CHCs growing. The Greater Boston area has a higher number of CHCs than other regions of the state due to the denser population and greater health needs. A high concentration of CHCs is necessary to help prevent and decrease unnecessary and preventable ED usage. A study was conducted in California to test if increased access to CHCs truly decreased ED usage, and they found increased CHC access and concentration in a geographic area was in fact associated with lower rates of uninsured ED usage (Nath, 2016). Because FQCHCs are funded through the ACA and other government waivers, they are required to report their health statistics publicly including usage by age, race, insurance type, and service (HRSA, 2017). Clear trends are visible for increasing CHC usage in Massachusetts since the ACA, but a relationship analyzing CHC use and corresponding ED use before and after the ACA in Massachusetts has yet to be established. Recent studies analyzing the same question, such as the 2019 Nath study for California, found that increasing FQCHCs in a geographic area decreases ED usage 26-35% in uninsured individuals (Nath, 2019). This paper aims to identify if there is a statistical significant increase of CHC usage and decrease of ED usage after the ACA came into effect in Massachusetts.